
Epic, Meditech, and Oracle Health environments are often the most controlled part of a hospital. But ransomware doesn’t need the EHR to shut down care. If clinical devices, building systems, shared services, or lab feeders are disrupted, downtime becomes a patient safety event. Zentera extends Zero Trust enforcement to these exposed systems - fast, agentless where needed, and without redesigning your network.
Verified access to only the applications and systems required for care delivery.
Granular, controlled connectivity without broad VPN reach.
An overlay that helps you see what’s talking and enforce what’s allowed—without redesign.
Clinical devices, building systems, shared services, lab/pharmacy workflows, and research environments.
Identify the non‑EHR systems most likely to cause care disruption if compromised—and prioritize fast containment.
Inventory and map dependencies for exposed domains: clinical devices, building systems, shared services, lab/pharmacy/imaging workflows, and vendor pathways.
Choose the first scope (one facility, one campus, or one “critical dependency cluster”).
Add enforcement without disrupting care; no multi‑quarter segmentation project required.
Deploy Zentera as an overlay and place enforcement where it fits: inline/agentless for fixed‑function assets and lightweight agents where supportable (e.g., on servers/workstations that broker access).
Connect to identity sources (IdP/Directory) and your logging pipeline.
Replace broad “zone access” with who/what is allowed to reach each critical dependency.
Create least‑privilege policies for the initial scope: clinician access, vendor access, service‑to‑service, and admin paths.
Start with a clear allow‑list for the workflows that must function (lab → interfaces, pharmacy → dispensing, facilities → monitoring, etc.).
Contain disruptions before they spread. Turn a hospital‑wide outage risk into a manageable, isolated event.
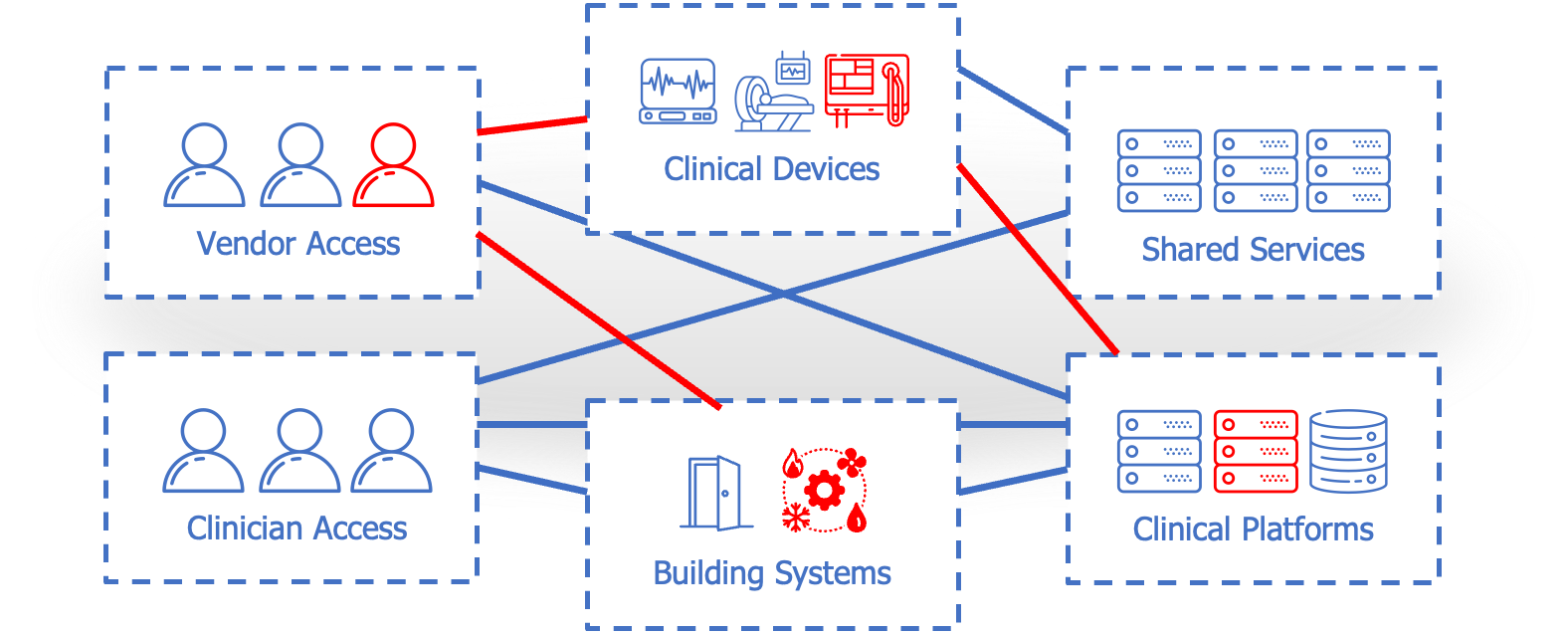
Enforce identity‑based connectivity and segmentation to block lateral movement between domains (devices ↔ shared services ↔ clinical platforms).
Reduce reliance on VLAN/firewall exception sprawl by enforcing policy at the overlay layer for the protected scope.
Prove value quickly (days, not quarters), then expand to the next priority system or site.
Validate workflows with clinical ops and IT, tune policies, and expand scope incrementally: one dependency set, building, clinic, or acquired site at a time.
Export enforcement signals to SIEM/SOAR and operationalize alerts for unauthorized access attempts.
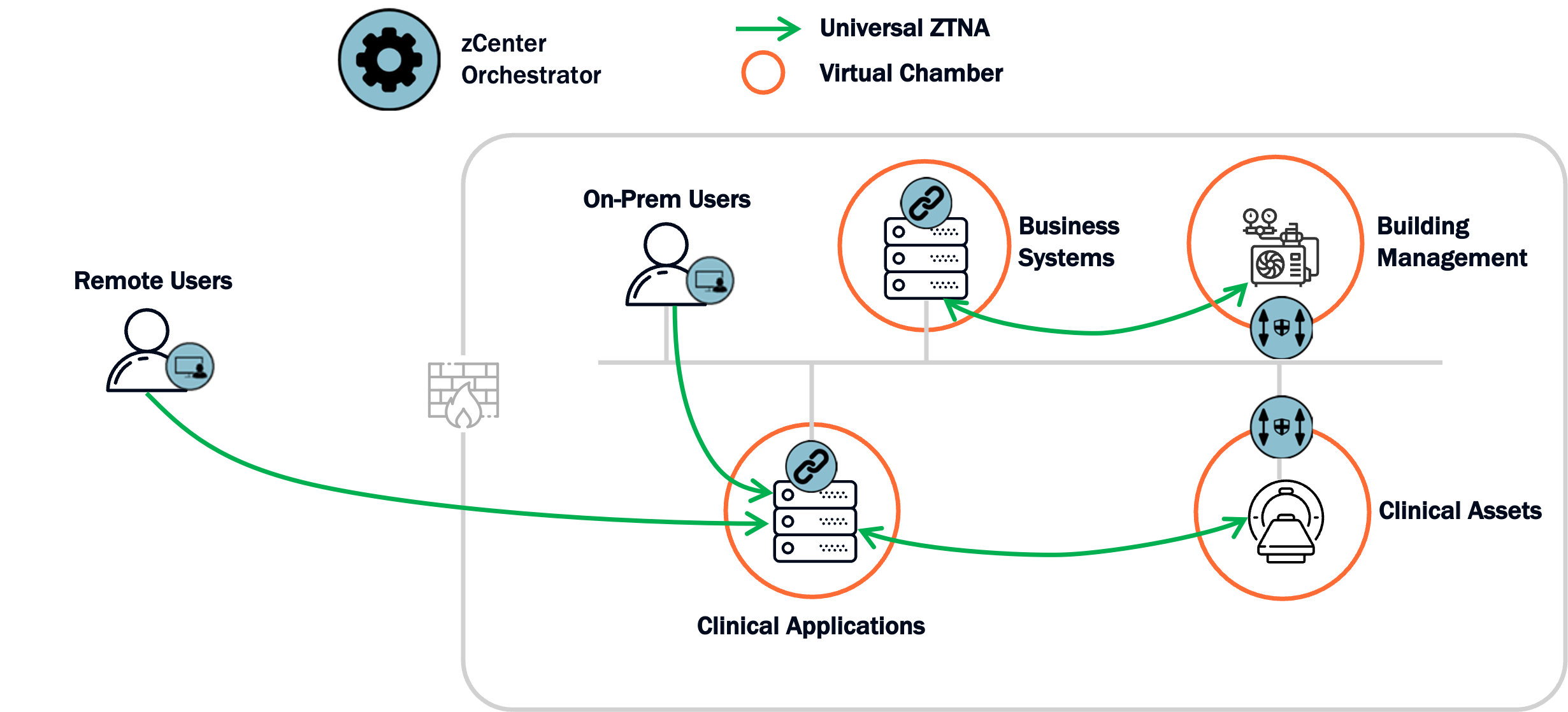
This architecture shows how Zentera overlays the healthcare environment and enforces least‑privilege connectivity between clinicians, vendors, clinical platforms, shared services, clinical devices, and building systems—reducing lateral movement and containing blast radius
Verified clinician and vendor access decisions replace implicit trust.
Zentera enforces allowed connectivity for the protected scope, without network redesign.
Shared services, facilities systems, and clinical support workflows are tightened so disruptions don’t cascade.
Keep existing EHR governance; extend protection to what attackers use to stop care.